After an extremely challenging year for healthcare systems, there are now opportunities to improve financial and clinical performance as the country begins to normalize.
In 2020, hospitals and health systems lost at least $323 billion and physicians were stretched to the breaking point. Unfortunately, the burden does not seem to be lightening for primary care physicians. Approximately 40% still feel the same level of strain due to COVID-19 that they felt a year ago. Finding additional ways to generate much-needed revenue, positively impact care, and reengage with patients is more critical now than ever before.
Preventive care services
It’s no secret that patients missed out on preventive care services due to the pandemic. Over the past year, 31% of patients in the United States delayed care and more than 50% of seniors canceled existing appointments. It is imperative to get back on track with preventive and routine care, especially for patients with chronic conditions.
Your physicians and staff should be proactively reaching out to patients, particularly Medicare patients, to schedule appropriate preventive care visits, such as Annual Wellness Visits, immunizations, and various cancer screenings. Scheduling a preventive care visit is a win-win for the patient and the physician. For the patient, it’s typically a no-cost visit that aids in the early detection and prevention of diseases, reduces the exacerbation of existing chronic conditions, and improves overall health and quality of life. For the physician, it’s a great opportunity to reengage with patients, create new revenue streams, and improve outcomes, which is especially important for improving performance under value-based care arrangements.
Health plan incentives
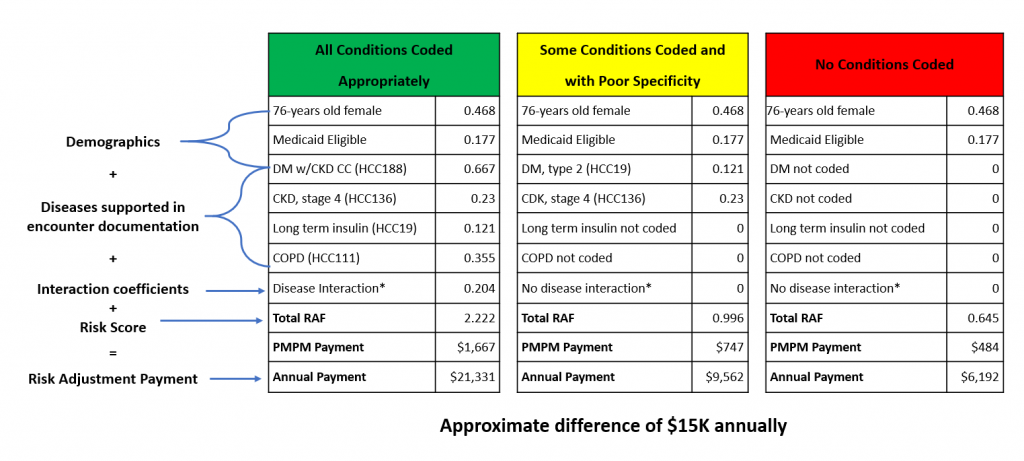
Health plans are eager to collaborate with physicians to achieve coding and quality of care goals. They need data and insights into their members and are willing to incentivize your organization to get it. Many payers offer programs that are free to your physicians and also pay incentives to capture real-time diagnostic coding that enables them to accurately risk-adjust their members. Some of these programs even help take the burden off of physicians and their staff by partnering with organizations that do the majority of the work, and they simplify the workflow by combining coding with preventive care services such as Annual Wellness Visits.
The timing for this could not be better. There is an emerging trend among health plans to shift from home assessments to PCP-centric prospective programs to better risk-stratify their members and address gaps in care. Given the established relationships patients have with their PCPs, prospective programs are often the most effective method for addressing gaps in care and ensuring alignment between medical record documentation and coding to the highest degree of specificity. Prospective programs permit real-time alerts of previously diagnosed conditions as well as those that are suspected. This ability to impact outcomes at the point of care is powerful.
VBC performance
Value-based care is designed to incentivize providers to improve outcomes in a cost-efficient manner. In other words, payment and quality of care are inextricably linked. The combination of driving higher utilization of key preventive care services and improving the accuracy of coding supercharges value-based care performance.
Unfortunately, many physicians lack the tools, resources, and experience to thrive in the value-based care model. Diagnostic coding and quality reporting are labor-intensive tasks and are predicated on a complex set of rules. In addition, EMRs are not equipped with all the necessary functionality and may not contain relevant health plan data, which results in an incomplete patient picture and suboptimal outcomes. Fortunately, there are solutions that include computer-assisted diagnostic coding technology, enhanced quality measure reporting, and clinical decision support at the point of care — all of which enable PCPs to improve outcomes and their financial performance under value-based care arrangements.
As we continue to move toward a new normal, physicians are beginning to see more patients for routine in-office visits, making this the perfect opportunity for patients and physicians to start reaping the numerous benefits derived from a refocus on preventive care and partnering with health plans on in-office programs to improve diagnostic coding and documentation.


Recent Comments